History 54 year old male with 3-year history of vocal problems. Teacher and sports coach, with recurrent hoarseness especially towards the end of semesters. Non-drinker and non-smoker with admitted voice abuse patterns particularly while coaching sport. Seen three years ago and diagnosed with "somewhat polypoid bilateral vocal nodules". Hoarseness resolved over the summer vacation. During recent vaction, problems did not resolve, and patient returned to the Voice Clinic. Previously told that it was unlikely that the problem would resolve in the long-term. Speech therapy has helped with vocal abuse patterns but has not succeeded in reslving the lesions. Initial examination The patient presents with very restricted vocal range, pitch breaks throughout this range, and persistent hoarseness. His voice exhibits a significant strained quality and some breathiness. The recording of the "Three Bears Passage", below, illustrates these characteristics.
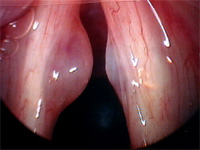
Video examination of his vocal cords revealed bilateral polypoid masses at the midpoint of the membranous vocal fold . The left mass is significantly larger than the right. The right mass (left on the images) is possibly a reactive nodular mass. Glottic closure is incomplete due to obstruction by the vocal fold masses. An "hourglass" glottis characteristic of bilateral lesions is noted, explaining the breathiness and strain of his vocal quality.
Vocal cord vibration is abnormal as noted in the stroboscopic endoscopic examination below. Mucosal closure does not occur suring the cycle, and mucosal movement is severely restricted due to the vocal cord masses on the medial edge. The mucosal movement which is present points to a lesion which is limited in its extent to the site of the mass. The lesion also appears to be superficial in nature due to the ease with which it moves superficial to the vocal ligament.
Operation The patient was placed under general anaesthetic and intubated. Using a suspended Dedo laryngoscope, the bilateral vocal cord masses were examined and photodocumentation recorded. Palpation of the lesions with a blunt probe revealed soft, polypoid masses which appeared to be superficial in nature, shown below.
The epithelial layer of both vocal folds was incised using microscissors, and a blunt probe used to establish a plane in the superficial layer of the lamina propria. microscissors were then used to excise the lesion in its entirety. Care was taken to avoid damage to the surrounding epithelium. See image above for immediate post-excision documentation. Postoperative Examination At his three month followup examination, the patient exhibits a remarkably normal voice. Most evidence of strain and hoarseness has disappeared, and pitch range is well within normal limits at 36 semitones. During conversation there are only occasional pitch breaks.
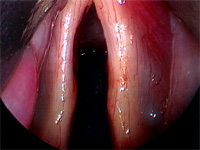
Video examination shows slight roughness to the medial edge of the vocal cords, especially on the left (right in the image) which was the site of the larger lesion. Closure is very good, and motion of both folds normal.
|