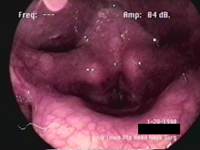
History 69 year old lady with 8 year history of sudden onset recurrent respiratory papillomatosis in the larynx and a total 13 laser excisions. Between surgical management of papillomas, her voice returns to reasonably functional level for approximately 8 months before recurrence of the problem. After her last surgery, approximately 7 months ago, she was very pleased with the outcome. Two months ago she reports having had flu, and she then lost her voice suddenly. She reports being aphonic for several weeks, and having a cough. She notes that recently her voice returned, but she is hoarse. Initial examination The patient presented with a moderately dysphonic voice, characterized by moderate roughness, mild breathiness, mild aesthenia and a moderately strained quality. The general pitch of her voice is judged to be abnormally low, although her pitch range is within normal limits at 25 semitones. Maximum phonation time is a low 14 seconds. the audio sample below illustrates the quality of her voice.
Videoendoscopy reveals that the patient has recurrence of laryngeal papilloma, giving the vocal folds a rough edge, and interfering with phonation.
Stroboscopy shows that the mucosal wave on both vocal folds is very restricted. Scarring from previous operations together with new papillomae can explain this.
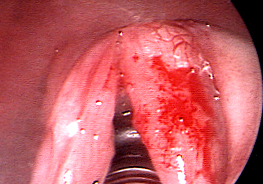
Operation The patient was placed under general anaesthesia with a 6.0 laser safe endotracheal tube. Under direct microlaryngoscopy, biopsies were taken using microlaryngeal instruments. Recurrent respiritory papillomatosis was found to diffusely involve both vocal folds. The subglottis and supraglottis were free of disease. Using a defocused carbon dioxide laser on 5 watts, continuous superpulse mode, th papillomata were ablated from both vocal folds , with only the left anterior commissure lased to prevent webbing scars. Result was photodocumented as seen below.
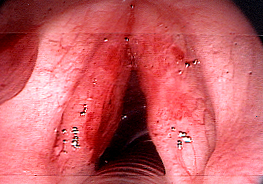
Postoperative Examination Two months after the operation, the patient returns for a followup examination. She reports an improved voice, and is judged to be mildly dysphonic with mild roughness, no breathiness, no asthenia, and no strained quality. This represents a very good result for this patient. Click here to compare the audio sample below with the preop sample.
Videostroboscopy reveals slightly rough irregular vocal fold edges, to be expected after so many surgeries. Mucosal action is much more pronounced, although far from being normal. The patient is satisfied with the result of the surgery, and her voice is adequate for her purposes, claiming that it does not impact negatively on her quality of life.
|