Nodules
case presentation
History
36 year old female mother of two with a 4-year history of intermittent hoarseness.
Nonsmoker, generally very healthy, regular exercise. Very talkative person with outgoing
personality and work which requires constant talking both to groups and on a one-to-one
basis. Reports that her family is also very loud in general. Gradual deterioration of
voice over the past few years. Some environmental allergies.
Initial examination
On examination the patient displays moderate dysphonia and a mild strained quality in
normal speech. During pitch-range exercises, voicing is intermittent but overall frequency
range relatively normal. Preoperative audio clip below illustrates these traits.
| Preoperative reading of the "Three Bears passage". Note
the moderate dysphonia and occasional pitch breaks, especially during phonation at higher
frequencies. compare this to the postoperative audio sample |
Videostroboscopic examination reveals bilateral vocal cord masses,
probably nodules, which impedes normal voicing. The vocal cords open and close normally in
prephonatory adduction as seen in the preoperative stills)
below. However, closure is not complete, due to the bilateral mass lesions.
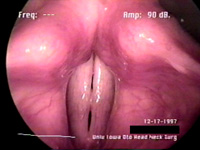
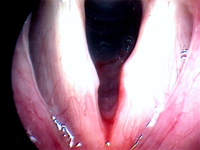
| Preoperative laryngoscope images. Left: maximally closed glottis
just before phonation. Right: maximally open glottis on inhalation. Note the incomplete
closure and characteristic hourglass shape due to the vocal fold masses. Click here to compare these images directly, and against
postoperative result. |
Stroboscopic viewing of the moving vocal folds shows vocal
cord motion inhibited by the presence of the masses. In the first video clip below, we see
phonation in the lower end of the pitch range. Due to the thickening of the vocal folds
required to produce low pitches, the nodules do not overly interfere with phonation. In
the second preoperative video clip, we see the pitch breaking and hoarseness noted in the
"baby bear" section of the audio recording above.
| Preoperative Strobed Video recording. This first clip is of low
frequency phonation. |
| Preoperative Strobed Video recording. This second preoperative clip
illustrates the pitch-breaking and hoarseness present particularly at high pitches. |
Operation
After about 6 months of voice therapy to try to relieve the nodules by
non-operative techniques, it was decided to intervene surgically and remove the nodules
using laryngeal microsurgical techniques. The patient was anaesthetised, and the nodules
removed in a micro direct laryngoscopic procedure. The medial edge of the vocal cords was
smoothed by cold dissection of the nodules, which were noticably larger in their inferior
extent than seen in the intraoperative photographs below.
| Intraoperative images. Left: vocal cords just before excision of
nodules. Right: immediately after microsurgical removal of nodules. |
Postoperative Examination
The postoperative audio sample below speaks for itself when compared to
the preoperative audio sample. This sample is from a ten-day
followup examination. The patient reports that she is able to sing again, and that her
voice seems almost back to normal. The sample clearly shows that removal of the nodules
has eliminated the pitch breaks which were occurring, and also shows an increased ease of
phonation.
| Postoperative audio recording. Compare this to the preop audio sample. Note the disappearance of pitch breaks and
strained quality of her voice. |
The postoperative examination shows that despite some residual scarring
from the surgery, normal vocal fold motion is restored. The still images below illustrate
the residual scarring, while the video clip show the relative unimportance of such minimal
scarring. Click here to compare these images directly, and
against preoperative examination.
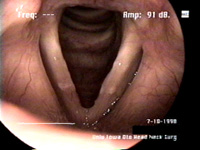
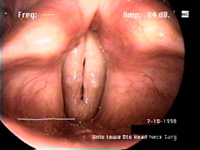
| Ten-day postoperative laryngoscope images. Left: Open glottis.
Right: closed glottis. We see that the vocal fold edge is not completely smooth due to
scarring from the surgical intervention, but that the nodules have been successfully
removed. |
| Postoperative Strobed Video recording. Some excess mucous present.
Note the signs of scarring from surgery: the right fold (left on the video) has a mucosal
wave which does not travel parallel to the medial edge of the fold, and the vocal fold
medial edge is also not perfectly straight. This does not seem to impede vocal cord
functioning to any important extent. |
|