History 68 year old cigar smoking male; reduced smoking because of voice problems; originally 10-15 cigars a day for 20 years, and cigarette smoking prior to that. "Lots of pepsi" (caffeinated) and maybe 3 cups of coffee a day. Minimal water intake (2 glasses per day). Clip shows extensive oedema of the vocal folds. Deterioration of voice since first diagnosis of Reinke's Oedema three years ago. Choking episodes prompted patient referral to Voice Clinic. Initial examination The patient displays an extremely limited pitch range of approximately 13 semitones, strained phonation onset, and frequent pitch breaks. The audio recording below, inspite of very poor audio quality (the harsh clipping noise) illustrates these attributes.
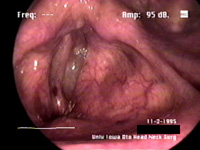
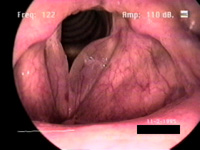
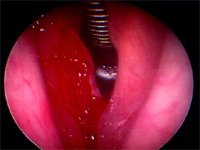
Initial examination of the larynx using a rigid endoscope (images below) reveals extensive bilateral oedema of the vocal cords, probably Reinke's polypoid degeneration. The left cord (on the right in the images) is seen to be more affected than the right. The reason for choking and inhalatory problems is immediately obvious: the vocal folds are very enlarged. Note vasularity especially on the right vocal cord (left in images!).
Video stroboscopy shows very assymmetrical vocal fold motion with false fold involvement on the onset of phonation. The right fold has a relatively normal appearance, with some mucosal wave. The left fold is completely oedematous, and has a very polypoid appearance. Closure is incomplete during the phonation cycle.
Operation The patient was placed under general anaesthetic and intubated with a laser-resistant endotracheal tube. The oedematous lesion of the left fold was found under microscopic investigation to have some overlying epithelial changes with leukoplakia, and was slightly firm to palpation. The right fold seemed normal with a small reaction-type nodule forming opposite the left vocal fold lesion. Using microsuction and laryngeal microscissors, a lateral cordotomy was performed and a microflap developed. The lesion was found to be superficial, and resection was carried out in Reinke's space. The left fold sample was sent for pathological examination, and was found to be polypoid.
Postoperative Examination At his two-month followup examination, the patient shows a considerable improvement. The pressing problem of airway restriction is no longer present, and voice quality has also improved. His pitch range is higher at 28 semitones (compared to 13 preop), and he is also trying to givre up smoking. The audio sample below gives evidence of a relatively normal voice, but still having an unusually low fundamental frequency.
The postoperative strobed video recording shows the right vocal fold (left in the video) having fairly normal motion characteristics, and a healthy mucosal wave. The left fold from which the oedema was surgically removed is all but immobile, with no surface movement at all, and involvement only at lower frequencies. The vocal system, however, is more symmetrical than preoperatively, and seems functions adequately.
|